Aqueous Shunt Implants for Glaucoma
The space between the cornea and the lens is filled with a clear fluid known as aqueous. Aqueous is responsible for maintaining intraocular pressure (IOP) which helps the eye to keep its shape.
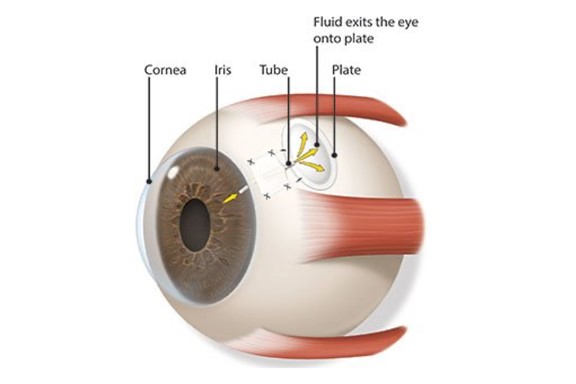
Intraocular pressure depends on how much fluid is made in the eye and how quickly it drains out of the eye. Sight loss from glaucoma is typically due to this pressure rising too high and damaging the optic nerve and leads to vision loss. An aqueous shunt is a small flexible tube which is implanted into the eye and improves the drainage of the fluid out of the eye. These shunts are made up of a small silicone tube (less than 1mm in diameter) attached to a plate.
Replacing the normal route that fluid would leave your eye, the fluid goes to a small reservoir under the outer layer of your eye (called a bleb) where the surrounding tissue can re-absorb it.
Different types of shunt are available. The two most common types are the Baerveldt Glaucoma Implant or Ahmed Glaucoma Valve. Other common names for this type of device are tube implant, glaucoma drainage implant or glaucoma tube shunts.
The Ahmed Glaucoma Valve contains a type of valve that helps to prevent very low eye pressure during the first few weeks after surgery. The Baerveldt implants do not contain valves but do have other advantages. For example, in the longer-term the Baerveldt Implant yields a lower average IOP than the Ahmed Implant which may be appropriate for patients who have a lower long-term IOP target. Because the Baerveldt implants have no valve, they must be blocked initially with a stent. The purpose of the stent is to prevent the shunt from draining excessively in the first few weeks after surgery and causing the eye pressure to be too low.

Baerveldt Drainage Implant
Mr Srikantha will make a pocket under the clear conjunctiva. The plate will be placed in this pocket and sit on the sclera. The tiny tube that is attached to the plate will be inserted into the front part of your eye. Aqueous fluid flows out of your eye through this tube, lowering the eye pressure. The fluid collects in a pool over the plate (called a reservoir or bleb). That fluid is absorbed naturally by your body.
After the procedure, your eye may be patched and you may need to wear the patch overnight. Plan to have someone drive you home after the surgery. Your vision may be burred for several days to a few weeks.
We will prescribe medicines to take for several weeks after the procedure. These medicines help prevent infection, discomfort and scarring.
You should not bend over, strain or lift heavy objects as you recover. Mr Srikantha will give you specific instructions and tell you when you can do these things again.
Most people with a glaucoma drainage implant will need to continue taking some glaucoma medications. Here at the Hampshire Eye Clinic, we will tell you which medications you should stop or continue.
You will need to see us a few times in the weeks after surgery for follow-up care. Be sure to keep these appointments.
FAQs
An aqueous shunt may be an appropriate course of action for patients for whom drop treatment has been ineffective or is unsuitable, or a previous surgery has not succeeded in controlling intraocular pressure. It may also be recommended as the first course of action in your glaucoma treatment. Ultimately it is a decision to be reached after discussing your condition and its progression with us.
As is typical for eye surgery, the eye may appear red or swollen temporarily. Similarly, the eyelid often droops. This generally resolves over a period of weeks to months. The aqueous shunt itself should not be visible on the outside of the eye. The tube is made of transparent silicone and is only 1-2mm long and should not be visible to the naked eye.
When the shunt is functioning normally, the drained fluid accumulates in a pocket known as a ‘bleb’ on the conjunctiva. This ‘bleb’ is positioned far back behind the eyelid so cannot usually be seen. The drained aqueous does not build up as it is absorbed by the blood vessels on the eye surface. Occasionally, the shunt or bleb can be seen in extremes of gaze, when the eye is looking very far down and in.
A small patch made of donor eye tissue, either from the sclera (the wall of the eye) or cornea is often used to keep the shunt in place. This is the only part of the operation that might be visible after surgery. Overall, an aqueous shunt implant should leave any noticeable changes to the appearance of your eye.
Aqueous shunt surgery generally lasts between one and two hours. It is generally performed under general anaesthesia, although local anaesthesia is also possible under certain circumstances. Patients who have their surgery under local anaesthesia will be awake during the operation but will have the option of requesting light sedation. The eye will be anaesthetised first with eye drops and then an injection of anaesthetic will be administered to the area around the eye. The injection anaesthetises the eye, preventing not only pain but also excessive eye movement during surgery.
During surgery patients are covered by a sterile sheet, or drape, which keeps the operation site sterile and also prevents patients from seeing any of the surgery. Patients will be aware of the surgeon working around the eyes, but it should not be painful. In the event of any pain or discomfort, calmly raise a hand and the surgeon will stop the surgery and top-up the anaesthetic if needed.
During the surgery, the drug Mitomycin C may be applied to the surface of the eye for a brief period of time (up to five minutes). Mitomycin C is a drug that was originally used to treat cancer, but it is also used in glaucoma surgery to reduce scarring. Scarring prevents the shunt from functioning in the long term, as it prevents the aqueous humour from being absorbed back into the circulation. The Mitomycin C is then washed away from the eye with sterile water so that no residual drug remains.
Patients are usually discharged home from hospital either the same day as the surgery or the following day. It is preferred that the eye be examined again one day after surgery.The eye is normally padded after surgery and the eye pad is removed the following day. If the unoperated eye does not see well, then the operated eye will not be padded. Instead, a clear shield will be placed on the operated eye so that it is still possible to see after surgery. The eye may be bloodshot for a few days following surgery. Patients are advised to ask a friend or relative to accompany them home after surgery, especially patients who have poor sight in the unoperated eye or those who have had general anaesthesia.
Patients are given a supply of post-operative eye drops on leaving the hospital and instructions on their use; these should last one month. The postoperative eye drops will normally need to be taken for two to three months. Patients are advised at each postoperative visit whether a change in the dosage of drops is required. The drops should not be stopped or the dosage changed without consulting the doctor. Patients are usually seen once a week for the first four weeks, and may be seen more frequently if the eye pressure is either too high or too low. Patients who find it difficult to visit their surgeon will likely be able to alternate post-operative appointments between their surgeon and local ophthalmologist.
It is important to avoid strenuous activity during the early post-operative period including swimming, tennis, jogging and contact sports. It is perfectly OK to watch television and read, as these will not harm the eye. Bending over can cause significant pain while the eye is still inflamed after surgery. Activities such as yoga that require head-down posturing should be avoided. Always consult your doctor before recommencing strenuous activity in the immediate post-operative period. Your progress and questions such as when you can return to work should be discussed during your follow-up consultations.
Overall, it takes two to three months for the eye to feel completely normal, although in rare cases it may take longer.
Most glaucoma surgical studies examine success rates over a five year period. With aqueous shunts such as the Baerveldt, the expected success rate over five years is now between 70 and 80 per cent. Although a sizeable proportion of patients achieve good pressure control without the need for continued glaucoma medication, many patients still require some medication to assist the shunt in controlling the pressure. In such circumstances, the medication required is usually less than was required before the surgery.
Severe complications are uncommon but are most likely to happen if the eye pressure drops very low or very quickly in the early post-operative period. A very low or an abrupt drop in eye pressure can result in a choroidal haemorrhage (bleeding at the back of the eye). However, this happens in less than one per cent of cases. If the pressure drops very low it may be elevated again either using an injection of a viscoelastic gel or a gas into the eye in the clinic, or by a return to the operating theatre to have the tube adjusted.
Roughly five percent of aqueous shunt patients require a return to the operating theatre in the first month after surgery for adjustment, either because of low pressure or high pressure. As with all eye surgeries, there is also a very small chance of infection, requiring further treatment.
Over the longer term, there is a risk that the tube implant may: develop a blockage (requiring further surgery to unblock the tube); erode (the surface conjunctiva over the shunt breaks down, requiring a repair operation); or rub against the cornea requiring further surgery to either move the tube so it does not rub or, in extreme cases where significant corneal damage has occurred, a corneal transplant may be required.
Aqueous Shunt Implantation has grown in popularity in recent years as techniques and technology have improved, leading to better outcomes and patient safety. It is now frequently used as a first-line surgical treatment for glaucoma.
Quality care in a relaxing surrounding


Book an appointment to see Mr Nish Srikantha at the Candover clinic in Basingstoke, or the Healthshare Clinic in Winchester.
Both locations are modern purpose built private hospitals designed entirely for patient well-being and comfort. The Candover Clinic is a stand-alone unit located on the Basingstoke and North Hampshire Hospital. The Healthshare Clinic on the outskirts of Winchester boasts a purpose built ophthalmic outpatients department and operating theatre offering the latest diagnostic and treatment technologies.