Trabulectomy
If you have glaucoma that isn't responding to drug therapies, then it is likely that you may require a surgical option to protect and preserve your vision.
Glaucoma, in it's various forms, all result from something blocking the movement of fluid in your eye through a structure called the trabecular meshwork. This causes an increase in pressure within the eye.
Creating a route for the excess fluid to escape is the obvious solution and Ophthalmologists have been doing surgery for almost 150 years.
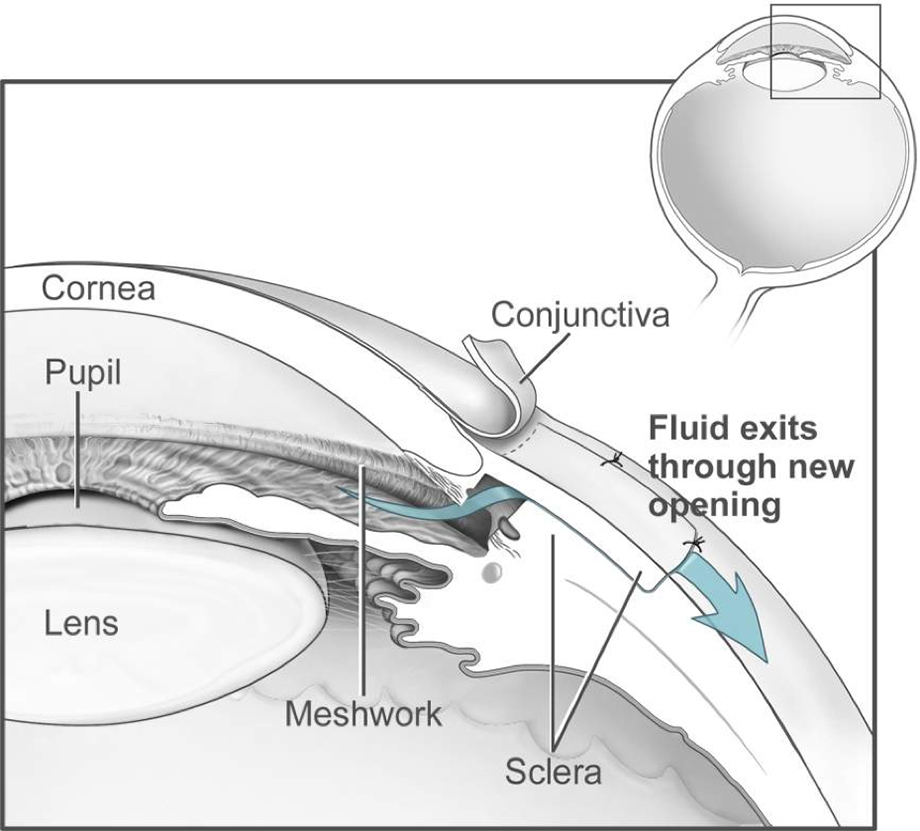
The modern Trabeculectomy is a technique developed by an English surgeon in the 1960's and its effectiveness means a much improved version is still one of the most common forms of surgery. Done under local or general anaesthetic, it involves removing a piece of the trabecular meshwork to allow fluid to leak from inside the eye, out through the wall of the eye and under the covering tissue (conjunctiva) where it slowly is absorbed.
The eye has two layers near the junction of the white and coloured part: these are the conjunctiva, a flexible tissue and the sclera, the strong white part of the eye.
Now there are variations on a theme here, Nish Srikantha is a Moorfield’s trained Glaucoma surgeon who practices the “Moorfields Safer Surgery Technique” which helps produce improved surgical outcomes following Trabeculectomy. He basically cuts and folds back a small window of conjunctiva and then a smaller flap is made in the sclera, under which a small hole is formed into the front chamber of the eye.
The flexible iris would plug up this hole from the inside, so a V shaped segment of iris is removed just underneath the hole to keep it clear. And that's it, a straightforward procedure. The flap is sewn in place with tiny releasable sutures that can be adjusted in the post-operative period to optimise intraocular pressure control. The fluid can escape through the hole into a space between the layers where it is reabsorbed and carried away from the eye, thereby reducing the pressure.
The location of the trabeculectomy is always under the upper eyelid. Once things have settled down, the signs of surgery are almost invisible as they are covered by the eyelid. In fact the only evidence of surgery is sometimes a small raised area, referred to as a 'bleb'. Many patients don't even notice they have one.
Post surgery your Glaucoma medication will be stopped immediately and within 3 months we will stop your post-operative drops. The good news is over two thirds of patients achieve their target pressure and are not taking medication 5 years later. Perhaps 20% of trabulectomies fail to control pressure after year 1 and require additional surgery. Is the fix permanent? Almost. Over time the effectiveness fades gradually and whilst there are patients still treatment free 30 years post-surgery, a few percent a year will find their pressures have crept back up to a problematic level.
Post surgery
For a few weeks after surgery, we actually prefer and expect the pressure in the eye to stay a little above our target pressure. There are two reasons for this; the first is that if we used sutures, removing or melting these reduces pressure; the second is we are fooling the eye into NOT healing the hole we created. We want the eye to believe nothing happened and it has already healed the opening shut. Usefully, the eye’s own aqueous fluid actually discourages healing, but taking a belt and braces approach we often add a strong anti-healing drug call mitomycin - C to prevent the internal opening from closing.
The patient's critical part in this is to put anti-inflammation eye drops on every 2 hours for a couple weeks and then slowly taper that off, which is the final and important step in making the operation work by keeping the hole open.
Other than not making a big enough pressure change, the main issues that come up after trabeculectomy are:
- Low a pressure (sometimes due to a leaking bleb). This can cause blurred vision and if very low the walls of the eye can start to 'sag' like a balloon losing air (hypotony maculopathy). This is a fixable issue but may involve more surgery to adjust the flap.
- Infection. A risk of any surgery, but rare in this instance, less than one in a thousand.
- Discomfort caused by the bleb area, and bleeding inside the eye. It takes about a year for the nerves to regrow and during that time, things can feel odd. This usually resolves by itself, maybe with the help of eyedrops and we rarely have to revise a bleb.
As with all surgery, there are those for whom it works brilliantly and those in whom it’s unlikely to win but worth the attempt. The success rate is higher in eyes without past surgery and in older persons. That's right, the older you are the better the outcome. This is down to your slower healing response. For reasons that aren’t fully understood but can be explained, some ethnicities do better than others with this surgery.
Quality care in a relaxing surrounding


Book an appointment to see Mr Nish Srikantha at the Candover clinic in Basingstoke, or the Healthshare Clinic in Winchester.
Both locations are modern purpose built private hospitals designed entirely for patient well-being and comfort. The Candover Clinic is a stand-alone unit located on the Basingstoke and North Hampshire Hospital. The Healthshare Clinic on the outskirts of Winchester boasts a purpose built ophthalmic outpatients department and operating theatre offering the latest diagnostic and treatment technologies.